| I
began this investigation expecting to find that the Sierra Leone
Government, my government, was wholly responsible for the disaster
unfolding in our country. The facts were indisputable: the outbreak had
started in the neighbouring republic of Guinea and our government
had had two full months to prepare before the first case was discovered
in Sierra Leone. And yet when Ebola entered, it swept through the
country with ease, almost as if we were defenseless. From the start
goverrnment figures were consistently lower than WHO's, and no one in
authority would acknowledge the seriousness of the situation, even when
we began to hear reports of entire villages decimated. Hundreds died,
perhaps even thousands, no one knows. Eventually the goverrnment
panicked at the scale of the emerging catastrophe, and once again we
had to run to the international community for rescue. Once again our
nation is threatened. Suitably patronizing and magnanimous, the world
outside Africa is responding. Meanwhile, the Guinean government,
although hard hit, has battled valiantly against the disease and has
managed to contain it to some extent. In two short months, from May to
July, our numbers of Ebola dead and crippled had risen from zero to far
outstrip theirs. This was the difference between a sober-minded
government and an incompetent one. This was how I saw it when I started
this work. Our
chronology begins with a terse statement on the
WHO website Ebola section
(https://www.who.int/csr/don/archive/disease/ebola/en/), dated “The
Ministry of Health (MoH) of Evidently
the outbreak had started some time before
this and the authorities in 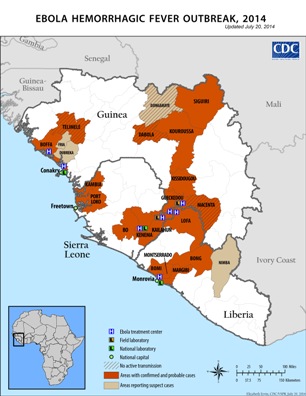
At
this point the information on the website
portrays a remarkably rapid response. The update of
March 26 reports that Ebola had been
confirmed in eleven blood samples by three separate laboratories, in
By
March 27 four cases of Ebola had been confirmed
in All affected countries appeared keenly aware at this point of the possibility of a wider outbreak. On March 27 WHO reports: “WHO
has alerted countries
bordering On
March 30, Contact
tracing was very strong in Especially
in its early stages, Ebola has symptoms that are similar to those of
many other diseases, and it must be confirmed by sophisticated
laboratory testing of blood samples. Initially,
samples from The WHO update of April 5 says (MOHSW here refers to the Liberian Ministry of Health and Social Welfare): "At
the request of the MOHSW and
WHO, the Metabiota Laboratory in This decision to put Metabiota in charge of lab testing in Liberia (and to effectively do the same in Sierra Leone) appears in hindsight to be more than a little curious, even foolhardy, even bizarre. This was a small, new organization with little experience in the region. Testing for the various strains of the Ebola virus is a sophisticated, highly specialized business. Even with all the right equipment the results can still be difficult to interpret, and experience is required. Metabiota was a new, for-profit organization with investors to satisfy. As far as I can tell from their documentation, they do not even have an independent laboratory of their own. By contrast, the Guineans were using the world-famous Institut Pasteur, founded by Louis Pasteur and credited with 10 Nobel prize winners and Germany's largest institution for research in tropical medicine, the Bernard Nocht Institute, federally funded. So the Liberians began using their new US laboratory, installed "at the request of the MOHSW and WHO" in the middle of the crisis. WHO reports on April 17 that , “The MOHSW commissioned a new ebolavirus laboratory on 16 April in collaboration with Metabiota.” All the while, the crisis had been eating into Guinea, with 109 lab-confirmed cases from six districts and many more clinical cases. All the lab testing was being done by two European installed labs within the country (one in Gueckedou and one in Conakry) and by the three partner labs mentioned earlier, all Europe centered. Meanwhile, two suspected cases of viral hemorrhagic fever in Sierra Leone were confirmed as Lassa Fever, not Ebola, by the lab in Kenema on April 7. The
Guinean authorities were working hard to contain the disease,
with significant help from international partners.They
would eventually trace several thousand contacts of confirmed cases,
one of the key steps to eliminating transmission of the disease. By
April
25 this work looked as though it might be starting to pay off. WHO
reported that the epidemiological situation had improved considerably, with four
affected districts not recording any
new cases for more than 21 days, the figure taken as the incubation
period of
the disease. In its May 2 update, the WHO reported that the number of suspected cases in Over the next several weeks the picture presented was one of steady improvement in the situation. The outbreak appeared to be ending. There was one ominous note on April 25 repeated and amplified on May 8: "As of 7 May, no cases of
EVD have been confirmed in Sierra Leone. From 16 March to 7 May 2014,
the Ministry of Health and Sanitation (MOHS) of Sierra Leone has tested
106 patients presenting with a VHF-like illness for EVD and Lassa
fever. No cases of EVD have been detected using ebolavirus PCR assays
while 10 patients have been confirmed with a Lassa fever virus
infection. Lassa fever is endemic in Sierra Leone"
This
surely should have sparked alarm, but apparently it did not.
106 samples collected
and tested. For what reason? The patients must have had symptoms
consistent with viral hemorrhagic fever. All 106 tested
negative for Ebola. Really? At a time when the disease was raging in
Guinea and all the signs now indicate it was also raging in Sierra
Leone and Liberia. In the same period Table: Cumulative lab-confirmed Ebola cases. * Table gives cumulative laboratory-confirmed Ebola cases from the last WHO update before the date indicated, except for week 8, May 20, where the update for May 23 was used.
On
May 12, In
its May 15 update WHO reported no new cases in As
late as May 24 WHO reports the situation
in On
May 28 cases from Sierra Leone suddenly spring up in the WHO updates
and mushroom in the coming weeks,
followed by a similar pattern in Liberia. The chart below and table
above depict the cumulativ From
numerous internet references, it's not hard to piece together a rough
outline of the Metabiota story in Sierra Leone: The US Department of
Defense contracted the company to assist in the Ebola outbreak. On
March 24, just as the outbreak is being announced by the WHO, two
officials from the company, Dr Joseph Fair and Dr Jean Paul Gonzalez,
take leave of Sierra Leone's ambassador to
the US, Bockarie Stevens. Ambassador Stevens is very supportive of
their mission and
hopeful that they will eliminate Ebola. The scientists are leaving with
a substantial quantity of reagents and other materials that are
essential in and specific to the testing of the various types of Ebola.
Metabiota is using a new type of test, real-time testing, possibly
invented by the company itself, as opposed to more conventional
methods. The Kenema lab, which had been in existence for years testing
for Lassa fever, appears to be using the conventional method. Somehow
Metabiota gains sway over the testing procedures at Kenema, to the
extent that only a few days after the arrival of the two officials in
Sierra Leone, they are invited by the WHO to set up the lab in Liberia.
For
eight critical weeks as the outbreak rages in Guinea these two
labs fail to detect a single case of Ebola, even though six cases of
Ebola in Liberia had previously been confirmed by the Guinean European
labs.There must have been some disagreement at the Kenema lab with the
scientists who favoured the conventional
method. Tulane University and Harvard University were the leaders in a
consortium of American
institutions that had been working at the lab on Lassa Fever for
several years. One could speculate on professional rivalry between
Tulane and the newcomers, Metabiota. At some point it was
resolved that both methods would be used to test incoming
samples (https://mysierraleoneonline.com/sl_portal/site/news/detail/2525
).
Only after this, on May 28, was it possible to confirm that Sierra
Leone indeed had cases of Ebola. Only after this could all the
Ebola-specific measures be implemented by government. On July 23 there
was the much discussed decision reported on the Sierra Leone Ministry
of Health Facebook page that Tulane University should stop Ebola
testing. The conflict between the two testing methods and two groups
appears to still
not have been fully resolved. It was discussed during a meeting of
Sierra Leone's Ebola Emergency Operations Center aired on national
television on Monday August 11. Metabiota appears still to be testing
samples for Ebola at the lab in Kenema. This
article does not seek to absolve the Sierra Leone government of blame.
National governments have to be held responsible for the health of
their citizens. The ministries of health of both Sierra Leone and
Liberia should have resisted efforts to engage an untested private
company on such a critical mission and should have been more skeptical
of its results. The Sierra Leone health authorities, if they had been
doing their jobs, should surely have picked up that there was an
alarming pattern of deaths in Kailahun, and that this could only, or at
least most likely, have been due to Ebola. But the WHO-approved labs
were telling the government here and in Monrovia that there was no
Ebola. We have heard many times during this epidemic talk of "fragile
countries", "weak health systems", "poor infrastructure", etc. If WHO
gives its blessing to. indeed appoints, a laboratory to do
sophisticated lab tests beyond the capabilities of these "weak"
national governments then WHO shares responsibility for the results of
those tests. It would be extremely interesting to find out who paid for
these tests, how much was paid and who authorized payment. I have no
means of doing that. It would be extremely interesting to find out more
about Metabiota, and what exactly they have been doing at the Kenema
lab, and how exactly they came to set up the Liberian lab in the middle
of this crisis. I suspect strong commercial and professional rivalry
between the
American interests that dominate in Kenema and the European
labs that were working with the Guineans, but I don't have details. I
have read all the internet accounts of US Department of Defense funding
for Ebola warfare research, although I make no claims here of anything
other than technical incompetence in the lab tests. I do appreciate that there are some organizations, even commercial enterprises, that are doing important work in the area of Ebola research, work that will hopefully lead to a vaccine and/or cure. And in order for these things to happen, at some point there needs to be human testing of the new medicines. These areas need to be entered into with great caution and under the strictest supervision. Not to do so, to allow fledgling companies seeking profit to enter these areas with abandon, invites the kind of disaster we see unfolding in West Africa.
© 2014 Paul Conton
|
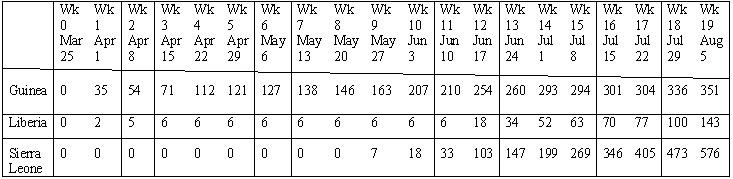
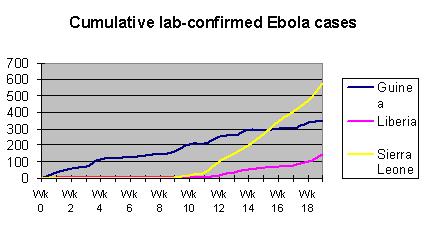 e
number of laboratory confirmed Ebola cases
by country over the course of this outbreak. Liberia's situation does
not look as bad as it actually is, because Liberia has a large number
of probable and suspected cases that never went through lab
confirmation. Liberia's actual position may in fact be more dire than
Sierra Leone's. Looking at the neighbouring Guinean situation, it's
hard to believe that Ebola was not present in the other two countries
long before May 28. Ebola was present, eating its way into our nations.
If it had been detected early it could have been contained, as the
Guineans managed to do, although they themselves have been affected by
re-infection from Sierra Leone and Liberia.The failure to detect early
caused the disease to mushroom in all
e
number of laboratory confirmed Ebola cases
by country over the course of this outbreak. Liberia's situation does
not look as bad as it actually is, because Liberia has a large number
of probable and suspected cases that never went through lab
confirmation. Liberia's actual position may in fact be more dire than
Sierra Leone's. Looking at the neighbouring Guinean situation, it's
hard to believe that Ebola was not present in the other two countries
long before May 28. Ebola was present, eating its way into our nations.
If it had been detected early it could have been contained, as the
Guineans managed to do, although they themselves have been affected by
re-infection from Sierra Leone and Liberia.The failure to detect early
caused the disease to mushroom in all